Emergency Scan
2–3 secondsCritical-only fast pass. The triage layer sweeps the volume and flags emergent findings within seconds, before a clinician opens the case.
First product · Abdominal CT
An end-to-end clinical AI workstation for abdominal CT. Scans are triaged by emergency severity, run through a pathology and anatomy pipeline, and surfaced to the doctor as anatomy-validated, explainable findings inside a reviewable report.
What Atlas is
Most imaging AI detects one pathology. Atlas runs a six-pathology emergency triage layer, anatomy segmentation, a doctor-editable report, and a per-case AI chat, all in one viewer, built to deploy on hospital infrastructure, Europe-first.
How a scan moves
Cases load by importance. The most emergent scans rise to the top of the queue. Two passes run: a critical fast-pass and the full pipeline.
Emergency Scan
2–3 secondsCritical-only fast pass. The triage layer sweeps the volume and flags emergent findings within seconds, before a clinician opens the case.
Full Analysis
20–30 secondsThe full pathology and anatomy pass. Findings are localized, organ masks built, anatomy cross-checks run, and a structured report drafted for review.
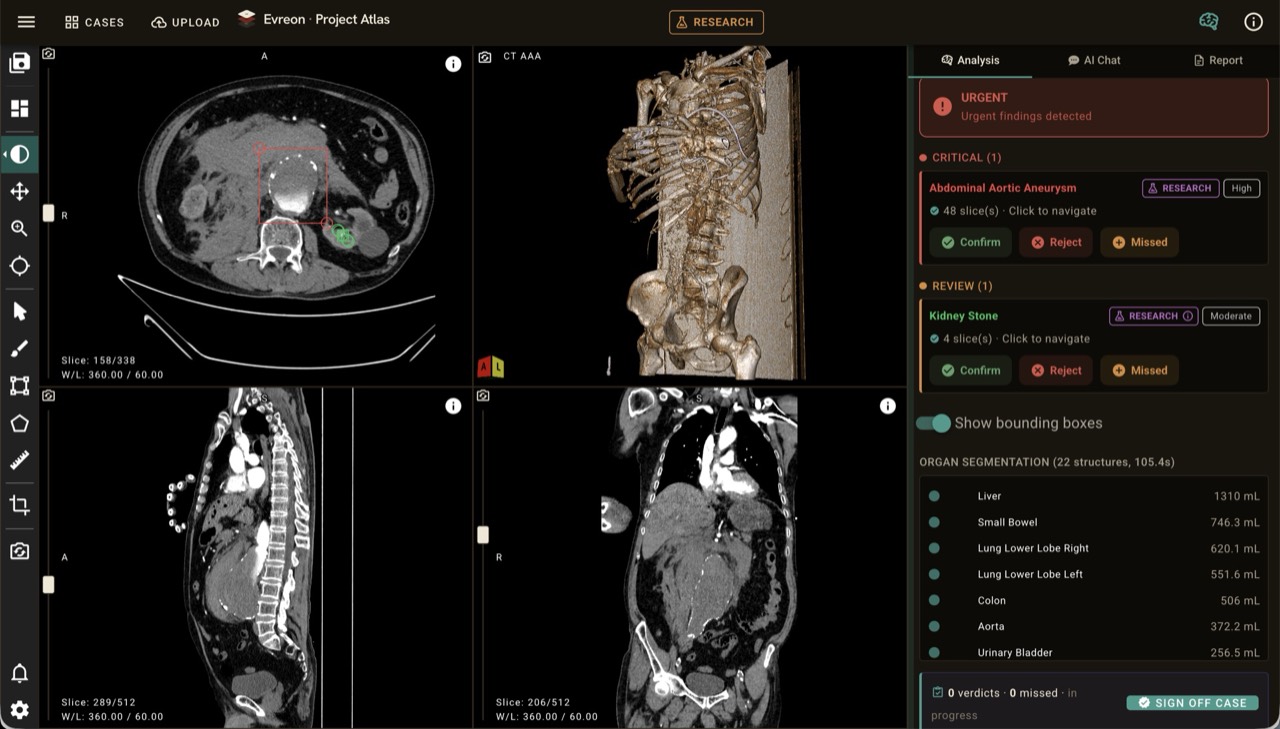
The viewer
The viewer's right panel has three tabs: Analysis, AI Chat, and Report, all wired to the same findings, anatomy, and slice references.
Try it yourself. Click the tabs to explore each panel
Critical (1)
Review (1)
Organ segmentation · 22 structures · 105.4s
Why doctors trust it
Explainability is the unlock. Doctors see why the model thinks what it thinks.
Hover any finding and a grid of de-identified training cases appears: real CT slices showing the same pathology. Doctors don't have to trust an accuracy number; they see what the model learned from.
Every finding carries a verified flag. Each detection is cross-checked against an organ mask and confirmed in the anatomically expected region. The gate is visible to the reader, not hidden in a pipeline.
Bounding boxes on the slice view and click-to-jump on every finding card. Spatial navigation is built into the finding, not a separate step.
How a case moves
A case enters from hospital infrastructure and is surfaced back to the clinician as an editable, anatomy-validated report.
Locked clinical scope
Internal validation
Peer-reviewed metrics from the published Atlas abdominal CT study, including external validation on a Stanford Merlin cohort. Kept separate from product, pilot, and demo claims.
Internal validation
Stanford Merlin cohort
Among detected cases
Strongest class
Atlas is a research-stage clinical AI system on the CE/MDR pathway, doctor-in-the-loop and research-use only. Pilots are free until clearance. We are opening free reference pilots with EU and Turkey hospitals.